
Theo Hiệp hội Đái tháo đường Hoa Kỳ (ADA) 2022, đái tháo đường thai kỳ (ĐTĐTK) là đái tháo đường được chẩn đoán trong quý 2 hoặc quý 3 thai kỳ mà trước khi mang thai tình trạng đái tháo đường không rõ. ĐTĐTK ảnh hưởng đến khoảng 14% các trường hợp mang thai trên toàn thế giới, đại diện cho khoảng 18 triệu ca sinh hằng năm. Riêng Việt Nam, tỷ lệ mắc bệnh từ 3.6 – 39% tuỳ theo tiêu chuẩn chẩn đoán và đặc điểm dân cư.

Nếu bạn bị đái tháo đường trong thai kỳ, không đồng nghĩa với bạn đã mắc bệnh từ trước lúc mang thai hoặc sau khi sinh con. However, Gestational diabetes puts you at increased risk of developing type diabetes 2 in the future.
Besides, if not treated properly, This condition increases the risk of developing diabetes in children, At the same time, it causes health complications for both mother and child.

Very rarely does diabetes during pregnancy cause obvious symptoms. The disease is only detected during routine examinations of pregnant women if symptoms of diabetes appear, include:
- Urinating many times a day;
- Tired;
- Blurred vision;
- Constant thirst;
- Snoring;
- Gaining weight too quickly compared to recommendations.
Causes of gestational diabetes
The pathogenesis of GDM is the result of pancreatic β-cell dysfunction on the basis of chronic insulin resistance during pregnancy under the combined influence of placental hormone factors..
When we eat, The body breaks down carbohydrates from food into a sugar called glucose. This sugar enters the blood, then moves to cells to provide energy for the body. An organ called the pancreas makes a hormone called insulin, Helps transport sugar into cells as well as reduce blood sugar levels.
During pregnancy, The placenta - the organ that nourishes and provides oxygen to the baby - secretes hormones that help the fetus develop. Một vài hormone trong số này khiến cơ thể thai phụ khó sản xuất hoặc sử dụng insulin hơn (còn gọi là đề kháng insulin).
Để giữ lượng đường trong máu ổn định, tuyến tụy của thai phụ phải tạo ra nhiều insulin hơn – gấp ba lần bình thường. Trong trường hợp tuyến tụy không thể tạo ra đủ insulin, lượng đường trong máu thai phụ sẽ tăng lên, gây ra bệnh đái tháo đường thai kỳ.
Your risk of developing diabetes during pregnancy increases if:
- Being overweight - obese before pregnancy;
- Gain weight very quickly during pregnancy;
- Have relatives (parents, brothers and sisters) have type diabetes 2;
- Have high blood sugar, But not enough to be diagnosed with diabetes. This phenomenon is called prediabetes;
- Có tiền sử mắc bệnh ở lần mang thai trước;
- Above 35 year old;
- Từng sinh một hoặc nhiều bé nặng hơn 4kg;
- Từng bị thai lưu, sinh con bị dị tật, sinh non;
- Đã hoặc đang bị hội chứng buồng trứng đa nang (PCOS).
Các nguy cơ khi mắc đái tháo đường thai kỳ
Đối với thai phụ bị đái tháo đường trong thai kỳ, các biến chứng sức khỏe có thể xảy ra là:
- Tăng huyết áp khi mang thai và tiền sản giật: These are two serious complications of pregnancy, can threaten the lives of both mother and child.
- Caesarean section: Because the baby is too big to be born normally, So you will likely have to have a cesarean section if you have gestational diabetes.
- Increased risk of premature birth.
- Increased risk of spontaneous abortion
- Increased risk of urinary tract infections.
- Having diabetes in the future: Bạn có nguy cơ gặp lại tình trạng này trong lần mang thai tiếp theo. Not only that, bạn còn có nguy cơ mắc đái tháo đường tuýp 2 khi về già.
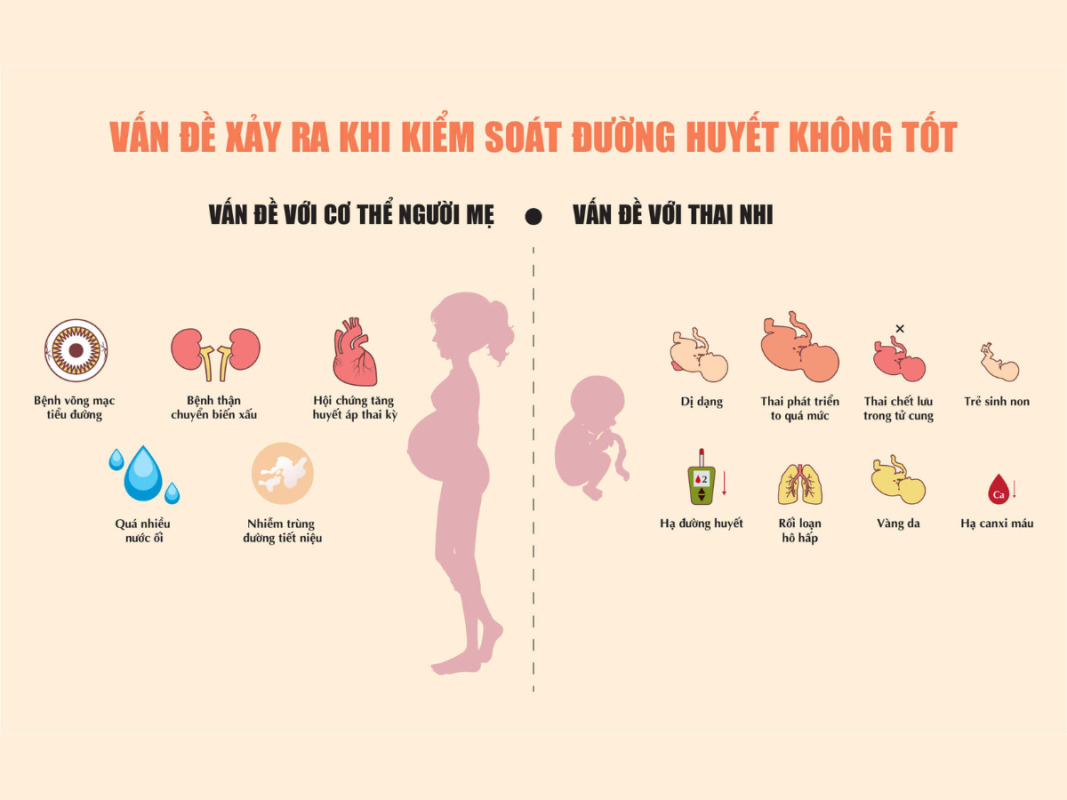
- Tăng trưởng quá mức và thai to: Lượng đường trong máu cao hơn bình thường ở người mẹ là nguyên nhân khiến thai nhi phát triển quá nhanh, leading to quite large birth weight (Usually over 4kg). A fetus that is too large will easily experience injury during birth or be unable to give birth normally.
- Premature birth: High blood sugar increases the risk of premature labor and giving birth before a pregnant woman's due date. Or pregnant women are advised to give birth early because the baby is too big.
- Severe difficulty breathing: Premature babies born to mothers with the condition are at risk of respiratory distress syndrome – a condition that causes difficulty breathing.
- Low blood sugar (hypoglycemia): Sometimes, Babies born to mothers with gestational diabetes will face low blood sugar soon after birth.. Not only that, Severe episodes of hypoglycemia can also cause seizures in your baby. It is necessary to feed the baby immediately or give the solution intravenously to bring the baby's blood sugar back to normal.
- Birth defects.
- Death immediately after birth.
- Increased red blood cells, newborn jaundice.
- Risk of obesity and type diabetes 2 when grown up.
- Stillbirth: Gestational diabetes, if not well controlled, can cause the fetus to die before or shortly after birth.
Recommended screening for gestational diabetes

Screening for GDM is recommended at week 24-28 pregnancy for all pregnant women without previous diabetes and lower screening tests 15 weeks of gestation in pregnant women with risk factors.
- “PROFILE” WHAT IS ABOUT HISMART MILK THAT MAKES BABY VERY NICE?
- Casino Pinko: reviews of cooperation with partners
- WHAT TO DO WHEN YOU ARE PREGNANT AND FIND OUT YOU HAVE GENE THALASSEMIA?
- HISMART AND MOM BOM SHOP BRING FAITH AND HEALTH TO DISABLED CHILDREN IN NAM DINH
- HISMART ACCOMPANIES WITH THE CHILDREN AT THE EVENT “HI AUTUMN”















